
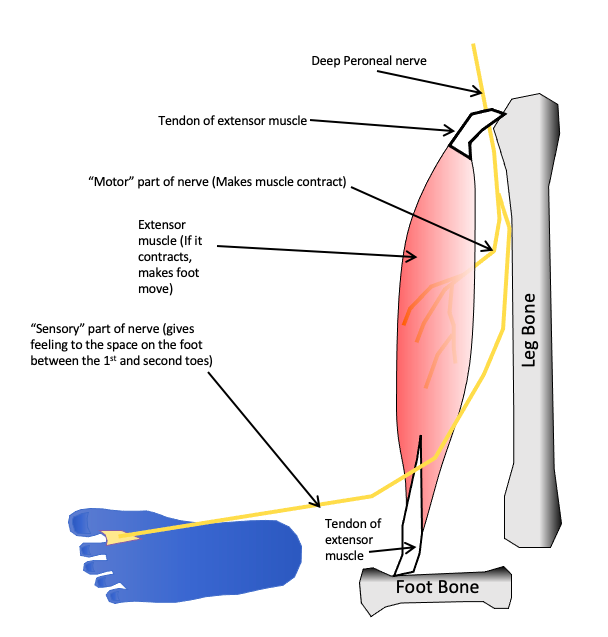
Muscles and tendons (collectively known as musculotendinous units), and nerves are soft tissues that are found throughout the body (see figure 1). Nerves electrically stimulate the muscles, which pull on tendons which move bones – this is how the body is able to move. Injuries to these units are frequent, with the arms, hands and fingers being the most commonly affected areas. Many injuries arise from some form of trauma, such as sports injuries, traffic accidents and work-related incidents. Most of these types of injuries heal well, although the time taken to complete this process varies considerably and depends on many factors. These include the patient’s age, the type and severity of the injury and the presence of any comorbidities that might affect healing. However, in some cases, functionality is never fully restored. This can impact on the patient’s ability to perform daily tasks and on their employability. As soft tissue injuries frequently occur in young, otherwise healthy, individuals, the implications of this can be serious.
In around half of all bone fractures or dislocations, there is some damage to the associated soft tissues. Often, these injuries can be diagnosed from the symptoms displayed and the circumstances surrounding the injury. However, in some cases, physical examination is not sufficient and an imaging technique or nerve conduction studies are required. Mobility does not necessarily imply the absence of injury, and it is important to definitively rule out conditions that may cause problems for the patient later on. Soft tissues do not show up on plain x-ray images, so a technique such as magnetic resonance imaging should be used instead.
One of the most important complications of soft tissue injury is damage to the nerves, which can happen by cutting, stretching, bruising, crushing or tearing. A patient report of abnormal sensation in the affected area, such as tingling or numbness, should raise the suspicion of nerve damage. Cutting, crush and tear injuries are usually the most severe – they may not heal spontaneously and may require surgical repair. Although nerves can regrow, they do so at a rate of only 1 mm per day. As function to an affected muscle must be restored within 18 months if permanent paralysis is to be avoided, continuous assessment of the return of functionality must be undertaken. If none is apparent after the first 3 months, a decision on whether to attempt surgical repair of the nerve must be made.
Tears in the muscle fibres or tendons, which connect muscles to bones, are often known as strains and are classified according to their severity. In mild strains, the fibres are stretched rather than torn, or tearing is limited to a small number of fibres. Moderate and severe strains describe tearing to most and all of the fibres, respectively. Complete tears usually result in a total loss of mobility in the affected joint. When the tear is not complete, movement is usually still possible, but this carries the risk that the damaged tendon will tear further, particularly if the joint is subjected to a high degree of stress. If the tendon tears completely, surgical intervention is often required to give the best chance of restoration of function. However, because tendons have a low metabolic rate, they heal more slowly than many other tissues and rarely regain their previous structural integrity and strength. To overcome this, the tendon thickens and stiffens, but this means that functional ability, and thus movement in the affected area, is reduced. As aging further alters the tendon’s mechanical properties, the prevalence of degenerative changes increases, potentially giving rise to a propensity to more damage in the future.
The treatment for many soft tissue injuries may involves immobilisation of the affected joint. However, if this is prolonged, it may become stiff and difficult to move. Furthermore, the muscles may shorten, leading to contractures, or waste away, and there is also the possibility of blood clots developing. As older patients have less strength and flexibility, and poorer balance, than younger patients, long-term problems are more common in this population, who also find it more difficult to compensate for the limitations caused by their injury. In some patients, full mobility is never restored. Therefore, patients should be encouraged to use the joint as soon as sufficient healing has taken place, and some form of prescribed physical therapy may also be useful.
Where a soft tissue injury leads to a permanent loss of function, the impact on the patient’s life can be severe. The upper limb, and in particular the hand, is vital to enable us to perform daily tasks, so any loss of mobility or dexterity is potentially devastating. If the nerves are affected, a long period of recovery is often required. Some patients are never able to return to their former employment and either have to be redeployed elsewhere or completely retrain for a different profession. This is particularly common in patients who formerly worked in construction or manufacturing, where a loss of sensation in the hand could be a substantial obstacle. In conjunction with the effects of the initial injury, the fear of unemployment and its financial implications can represent a significant psychological burden for the patient.
Further reading:
Bergmeister, K. D., Große-Hartlage, L., Daeschler, S. C., Rhodius, P., Böcker, A., Beyersdorff, M., Kern, A. O., Kneser, U., & Harhaus, L. (2020). Acute and long-term costs of 268 peripheral nerve injuries in the upper extremity. PloS one, 15(4), e0229530. https://doi.org/10.1371/journal.pone.0229530
Wu, F., Nerlich, M., & Docheva, D. (2017). Tendon injuries: Basic science and new repair proposals. EFORT open reviews, 2(7), 332–342. https://doi.org/10.1302/2058-5241.2.160075